

An Experimental Pharmaceutical Treatment for Long Covid (Part 1: Impact on Symptoms)
Part 1: Impact on Symptoms

For the past several months, I have been talking about and exploring the general hypothesis that microclots caused by the Covid Spike Protein are the primary event that causes Long Covid.
In examining those microclots and how they form in the body, we now understand that microclots are the result of TWO distinct mechanisms: the formation of abnormal amyloid microclots of fibrin AND platelet hyperactivation. We have reviewed the data showing that the Covid Spike Protein causes both of these effects and that both microclots and platelet hyperactivation are present in Long Covid patients.
We also asked the questions and reviewed the data about whether anti-coagulants and aspirin (a platelet activation inhibitor) can treat Long Covid. The answer for both these classes of drugs is that neither can alleviate Long Covid symptoms as a mono-therapy. Aspirin ALONE can decrease platelet hyperactivation at the molecular level, but does not alleviate the symptoms of Long Covid. Clinical use of anti-coagulants ALONE in patients with Covid seemed to have little effect and anti-coagulants have not been evaluated on a molecular level to see if they break up microclots.
The next logical question to ask is: What happens if you combine an anti-coagulant with a platelet activation inhibitor? Can that combination treat Long Covid?
Triple Anti-Coagulant Therapy as a Treatment for Long Covid
Fortunately, two great scientists and their team - Etheresia Pretorius, Douglas Kell, and their coworkers - have asked that question and done a study of what’s known as “Triple Anti-coagulant Therapy” in Long Covid patients.
Triple Anti-Coagulant Therapy combines a pharmaceutical anti-coagulant (apixaban) with two different platelet activation inhibitors - the pharmaceutical drug clopidogrel and aspirin.
But before I go any farther, I have to say one thing…
DISCLAIMER: The data that I am about to present and discuss has NOT undergone peer-review and has NOT been formally published in a journal. This information is from a preprint article that has NOT been peer-reviewed. Scientists can say a lot of things in a preprint that might not survive the scrutiny of peer-review.
So why am I presenting unpublished information and data to you? Two reasons:
I think this information is important enough that people need to see it, even if some of it might not hold up to peer review and
The authors (Pretorius, Kell, and coworkers) are highly reputable and have a strong publication track record. It’s unlikely they would fabricate data, or make false or unsupported claims.
I’ve included the link to the preprint website below, so you can look at the actual pre-print document and judge for yourself.
Now, let’s talk about the…
Experimental Pharmaceutical Treatment for Long Covid
Pretorius, Kell, and coworkers examined a cohort of 91 Long Covid patients (54 females, 37 males, average age 50+/-14), who they treated with Triple Anti-Coagulant Therapy. The patients were extensively evaluated both before and after the course of treatment.
Each patient reported their Long Covid symptoms before and after treatment. Prior to receiving Triple Anti-Coagulant Therapy, the most common Long Covid symptoms reported were fatigue, cognitive dysfunction, shortness of breath, and joint & muscle pain.
Blood samples were taken from the 91 patients before and after treatment. The blood samples were evaluated by fluorescence microscopy for microclots (thioflavin T, ThT) and platelet hyperactivation (CD62P & PAC-1 fluorescent markers). Prior to starting treatment, all 91 patients were confirmed to have microclots and platelet hyperactivation, the molecular hallmarks of Long Covid.
The duration of Triple Anti-Coagulant Therapy treatment for each patient depended on how long they had suffered from Long Covid. According to the pre-print, “Patients with ‘short’ Long Covid (symptoms less than 6 months) usually needed treatment for 2-4 months, which those with ‘long’ Long Covid (symptoms more than 6 months), needed 4-6 months (or longer) of treatment.”
Results from the Study
Finding #1: For each Long Covid symptom evaluated, >74% of patients saw that symptom resolve and no longer be present.
The full set of data is in the table below.
Let me walk you through one symptom, Cognitive Dysfunction, so you can understand the numbers below more clearly.
Let’s start with the “Patients with Symptom BEFORE Treatment” section (the yellow columns). For Cognitive Dysfunction, 82 of the 91 Long Covid patients (that’s 90%) suffered from cognitive dysfunction before starting the treatment.
Now let’s look at the “Patients with Symptom AFTER Treatment” section (the orange columns). For Cognitive Dysfunction, only 21 of the 82 patients (26%) still suffered from cognitive dysfunction after the treatment.
Finally, let’s look at the “Patients WITHOUT Symptoms AFTER Treatment” section (the green columns). For Cognitive Dysfunction, in 61 of the 82 patients (74%) the cognitive dysfunction symptom was resolved and was no longer present after completing the Triple Anti-Coagulant Therapy.

And Cognitive Dysfunction was the symptom that saw the least improvement. For all the other symptoms, the symptom resolved and was no longer present for >75% of all patients that entered the study suffering from that symptom. That means 3 out of every 4 people (or more) suffering from a given symptom got better.
The results for improvements of the symptoms are so good, Pretorius, Kell, and coworkers made this statement in the Abstract of the pre-print: “Following completion of the treatment, each of the different symptoms resolved in the majority of patients.”
That’s a pretty encouraging statement, even for a small study.
Finding #2: 80% of the Long Covid patients (73 of 91 patients) showed enough of an improvement in their Patient Global Impression of Change (PGIC) Scale to be considered “recovered” from Long Covid.
Following the conclusion of their course of therapy, the patients in the study rated their improvement using the Patient Global Impression of Change (PGIC) scale. The one-questions survey and the ratings scale are shown below:
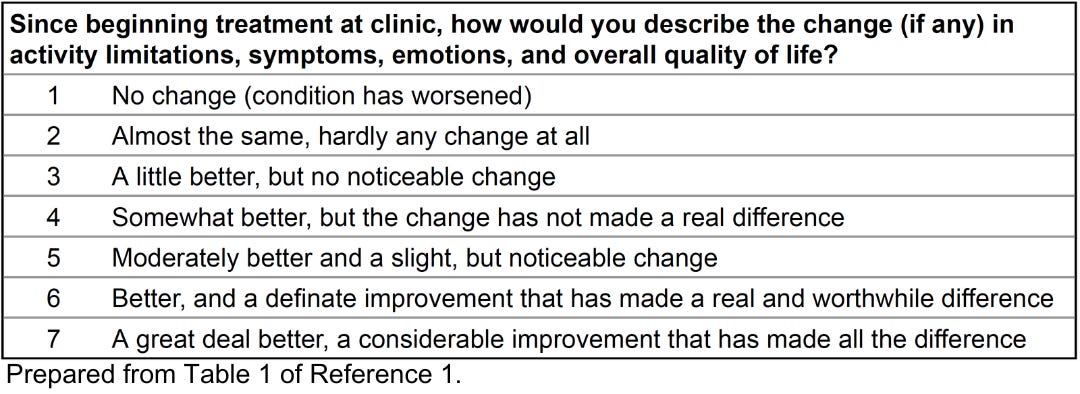
The data was stratified according to those suffering from ‘short’ Long Covid (symptoms less than 6 months) and those with ‘long’ Long Covid (symptoms more than 6 months). The individual patient scores were then plotted on a Histogram (see below). Patients with a PGIC score of 5-7 were judged to have “recovered” from their Long Covid. Patients with a PGIC score of 1-4 were judged to have “no or little” recovery. As can be seen from the data below, 80% of the Long Covid patients in the study (73 of 91 patients) reported PGIC scores of 5-7 and were therefore judged to have “recovered”. That’s a remarkable 4 out of 5 patients recovering from Long Covid on Triple Anti-Coagulant Therapy.
The median PGIC score for the entire population of 91 Long Covid patients was 6 - defined as “Better, and a definite improvement that has made a real and worthwhile difference”.
I think most Long Covid patients would find this result encouraging as well.

This summarizes the impact on symptoms of the Triple Anti-Coagulant Therapy in this study of 91 Long Covid patients from Pretorius, Kell, and coworkers. Remember this is a preprint - see the Disclaimer above and the Reference below.
In my next post, I’ll present more detail on the molecular mechanisms of action of the drugs that make up the Triple Anti-Coagulant Therapy, the effect of the treatment at the molecular level on microclotting and platelet hyperactivation, and the side effects that were observed during the study.
Stay tuned for that information and much, much more.
Leave me a comment below and let me know what you think of this post.
And to follow my research, subscribe to my SubStack!
Reference
Treatment of Long COVID symptoms with triple anticoagulant therapy. Research Square Preprint 2023, rs-2697680/v1. https://doi.org/10.21203/rs.3.rs-2697680/v1