

Can Aspirin treat Long Covid?
...by treating Platelet Hyperactivation?

Over the past couple of months talking about microclots and platelet hyperactivation in Long Covid, multiple people have asked the question:
“Can aspirin be used to treat Long Covid?”
Today I want to examine the common beliefs that people have about aspirin and how it could be therapeutically useful in treating Long Covid. Then I want to talk about the science behind aspirin, including its mechanism of action, and the limited data showing what aspirin does when taken by a person suffering from Long Covid.
Common Beliefs about Aspirin
Most people know that aspirin has been around for a long time and has multiple therapeutic uses, as well as some drawbacks.
Aspirin was originally discovered and traditionally used as a pain reliever. The origins of aspirin started with the use of Willow bark extracts as a pain reliever in folk medicine as far back as ancient Egypt. In the late 19th century, Bayer Pharmaceutical company in Germany prepared and started selling aspirin in pure form as an anti-inflammatory to treat pain and fevers. The pain relief dose of aspirin is 325 mg taken every 4 hours.
Once aspirin came into common use as a pain reliever, the drawbacks started to become known. The biggest drawback for aspirin is that it causes irritation and potential bleeding of the lining of the gastrointestinal (GI) tract, making its use discomforting or painful for some people. This drawback led to the development of other anti-inflammatory drugs (acetaminophen, ibuprofen) that most people now use.
After its fall from grace as a pain reliever, aspirin gained new life as a preventative treatment for cardiovascular diseases. Daily consumption of low-dose aspirin (generally 81 mg) promotes healthy circulation and prevents heart attacks and strokes. It’s thought to thin the blood, reduce blood clotting, reduce inflammation in the veins and arteries, and help maintain healthy blood flow in the circulatory system. Taken together, all these effects decrease the risks of heart attack and stroke.
Most people that suggest using aspirin to treat Long Covid are thinking about aspirin in the context of a preventative treatment for cardiovascular diseases. Since aspirin acts as a “blood thinner” and helps prevent/reduce clots, shouldn’t it help with the microclots found in Long Covid? As with most things, the answer is both Yes and No - keep reading below to see why.
The Science behind Aspirin
Aspirin, also known by its chemical name acetylsalicyclic acid, exerts both its anti-inflammatory and cardio-protective effects by inhibiting platelet activation.
Aspirin irreversibly inhibits the COX-1 and COX-2 enzymes that are found in platelets. When the COX-1/2 enzymes are activated, both thromboxane A2 (which promotes platelet aggregation) and prostaglandins (which promote inflammation) are produced, resulting in widespread platelet aggregation and clot formation in the blood, as well as diffuse inflammation in the endothelium of the blood vessels and surrounding tissues/muscles.
When aspirin inhibits the COX1/2 enzymes, platelet activation diminishes, as does the associated aggregation of platelets to form clots and inflammation. This happens when using the higher, anti-inflammatory dose of aspirin (325 mg).
At the lower cardio-protective aspirin dose, COX-1 is preferentially inhibited, blocking the production of thromboxane A2 and its accompanying platelet aggregation.
Aspirin, even low-dose aspirin, can inhibit platelet activation and aggregation, which should help reduce blood clots.
So can aspirin be used as a treatment for platelet hyperactivation in Long Covid?
In Long Covid, Aspirin prevents Platelet Hyperactivation, but NOT Microclots
In one of the papers studying microclots and platelet hyperactivation in Long Covid patients (Ref 1), data is included from patients that have been self-administering aspirin as a treatment.
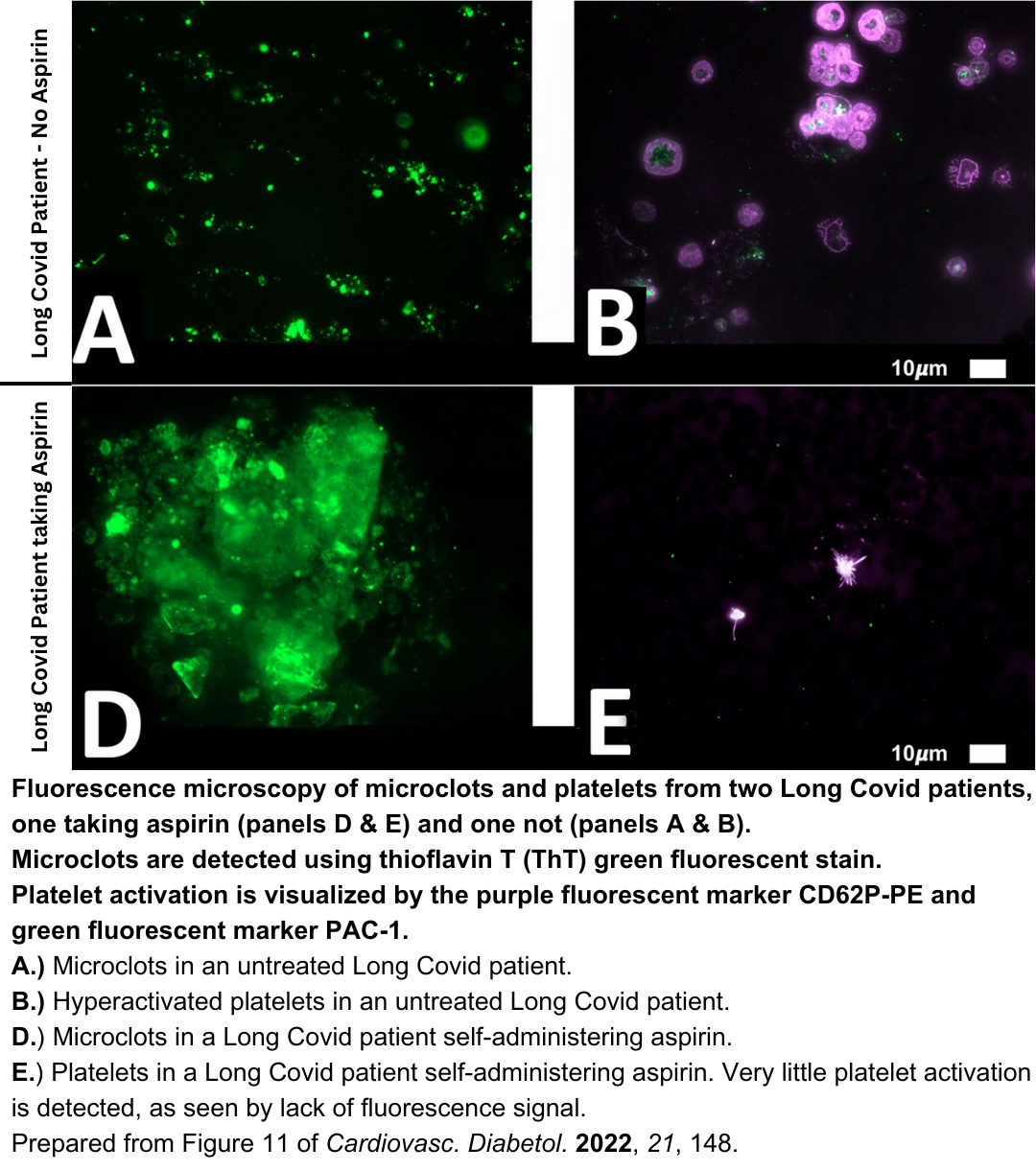
In Long Covid patients that have NOT been taking aspirin, typical microclots (amyloids of fibrin) and platelet hyperactivation, both caused by the Covid Spike Protein, are observed (panels A & B below).
In Long Covid patients that HAVE been taking aspirin, ONLY microclots are observed (panel D below). When the patients are taking aspirin, the platelets look normal and are NOT hyperactivated (panel E below), as normally seen in Long Covid patients.
So what conclusions can we draw about the use of aspirin to treat Long Covid?
Aspirin alone CAN reduce the platelet hyperactivation observed in Long Covid patients (panel E).
Aspirin alone CANNOT alleviate the symptoms of Long Covid patients, despite reducing platelet hyperactivation.
In patients that are self-administering aspirin, the Long Covid symptoms likely persist due to the untreated microclots, which are clearly still present in these patients (panel D).
The use of aspirin seems to parallel and is similar to the use of anticoagulants to treat Long Covid. Remember that anticoagulants ALONE cannot alleviate the symptoms of Long Covid, likely due to untreated platelet hyperactivation.
What’s Next?
So what happens if we use both anticoagulants and platelet activation inhibitors together?
That will be next week’s post. Stay tuned for the epic answer!
Leave me a comment below and let me know what you think of this post.
And to follow my research, subscribe to my Substack!
References
Prevalence of symptoms, comorbidities, fibrin amyloid microclots and platelet pathology in individuals with Long COVID/Post-Acute Sequelae of COVID-19 (PASC). Cardiovasc. Diabetol. 2022, 21, 148.